The Integrated Care System brings partners together to organize and deliver services that aim to promote prevention, improve health and wellbeing outcomes and to reduce inequalities for our population. Over the last few years, we have developed and refined the way in which the ICS is constructed, its membership model and how it operates. We have seen it emerge from the original concept of the Sustainability and Transformation Partnership and we are now on the verge of the next big step in our integration journey.
The Integrated Care Board is the statutory NHS body that has replaced the Clinical Commissioning Group (CCG) and has inherited a range of new functions delegated from NHS England. The ICB receives the NHS financial allocation for Herefordshire and Worcestershire and has the important role of allocating it out across services to ensure the best outcomes are achieved.
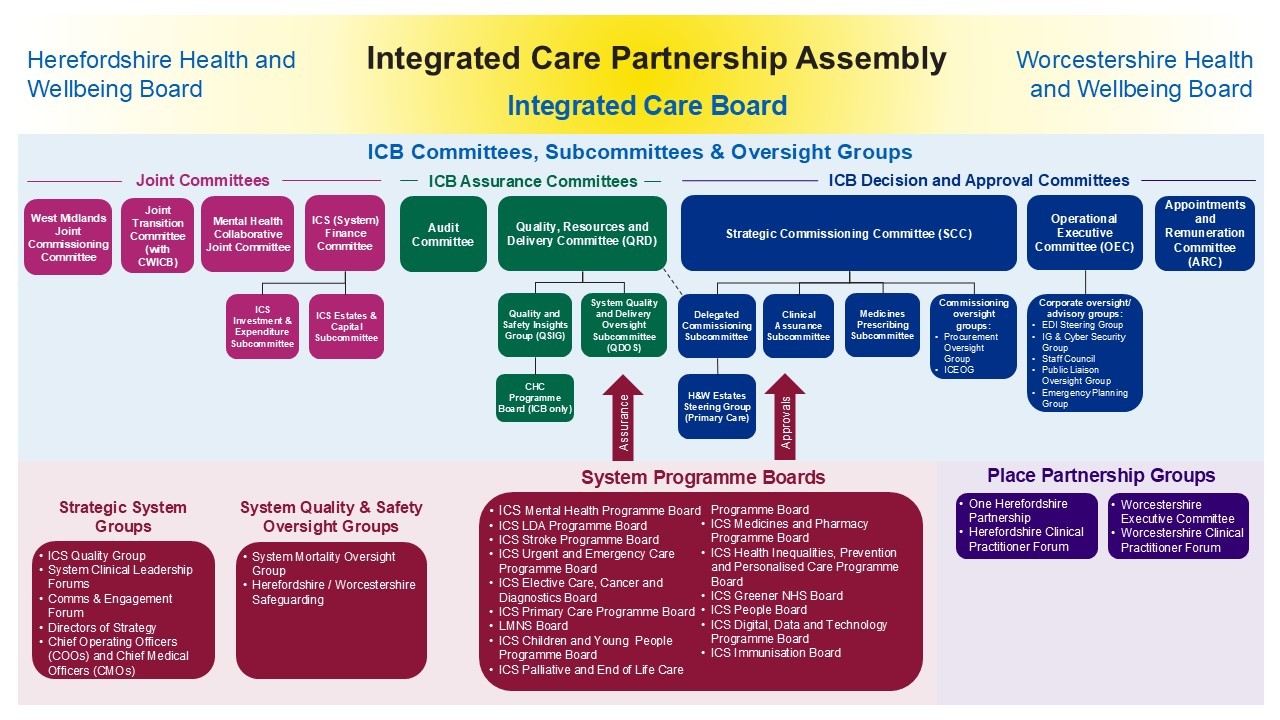
These documents illustrate the proposed operating model of the Integrated Care Board and how it interfaces with other parts of the Integrated Care System.
Our constitution sets out the arrangements to meet our responsibilities for commissioning a wide range of healthcare services for the people of Herefordshire and Worcestershire. It is the foundation of our organisation and clearly describes what we are setting out to achieve, and how we intend to achieve it. The Constitution sets out:
- Who we are as an organisation
- Who constitutes our Board
- How we form our Board and the standards those individuals must uphold
- How and when we make decisions (Please see Scheme of Reservation and Delegation, Standing Financial Instructions and Detailed Standing Financial Instructions for a full breakdown of delegated decision making arrangements)
- Who within the organisation has the delegated authority to make decisions on behalf of the organisation
- How we will manage conflicts of interest and standards of business conduct (Please see Conflicts of Interest Documents section below for more detail)
The ICB has established a number of committees in order to enable the organisation to effectively fulfil and oversee delivery of its functions.
The ICB committees comprise of:
- Appointments and Remuneration Committee (ARC)
- Audit Committee
- Finance Committee
- Joint Transition Committee
- Mental Health Joint Committee (MHJC)
- Non-Executive Member Appointments and Remuneration Panel
- Operational Executive Committee (OEC)
- Quality, Resources and Delivery Committee (QRD)
- Strategic Commissioning Committee (SCC)
The structure of sub-committees, system groups and programme boards that report into these committees can be seen in the Operating Model.
This Organogram is published in response to a request from the Secretary of State for Health and Social Care dated 9 December 2022.
The request asks Integrated Care Boards (ICB’s) to publish “the structure of teams within the ICB, including the number of staff in each team and at each grade and the total cost per team. This will help the public to understand how ICBs are structured including which roles report to others and also highlight the work that you are doing to develop integrated care.”
The figures in the chart relate to substantive (permanent) posts funded by the ICB Running Cost Allocation, a specific allocation covering the corporate administrative functions of the ICB. At any one time due to staff turnover, a number of teams may have vacancies or posts may be filled by temporary staffing whilst recruitment is underway, but the tables represent the staffing levels at present.
In addition to the directly employed workforce, additional corporate functions are supported by contracts with a local Commissioning Support Unit. These include elements of Business Intelligence, Finance, HR, Procurement, IT and Counter Fraud services. Staff providing these services are employed by the relevant partner organisation and are therefore excluded from this organogram.
Effective handling of conflicts of interest is crucial to give confidence to patients, taxpayers, healthcare providers and Parliament that ICB commissioning decisions are robust, fair, transparent and offer value for money.

